What causes shoulder pain?
Like many pain complaints, shoulder pain can have many causes and involve various processes, including traumatic injury (joint sprains, muscle strains, tendon tears), bursitis, osteoarthritis and frozen shoulder (adhesive capsulitis).
However, one of the most common presentations in the chiropractic clinic is moderate to severe shoulder pain with no known injury associated with the onset of pain. People often present already having had scans performed to reveal mild tendon changes or inflammation as well as bursitis…….but what is the cause?
To understand this, we need to look at the structure and function of the shoulder complex.
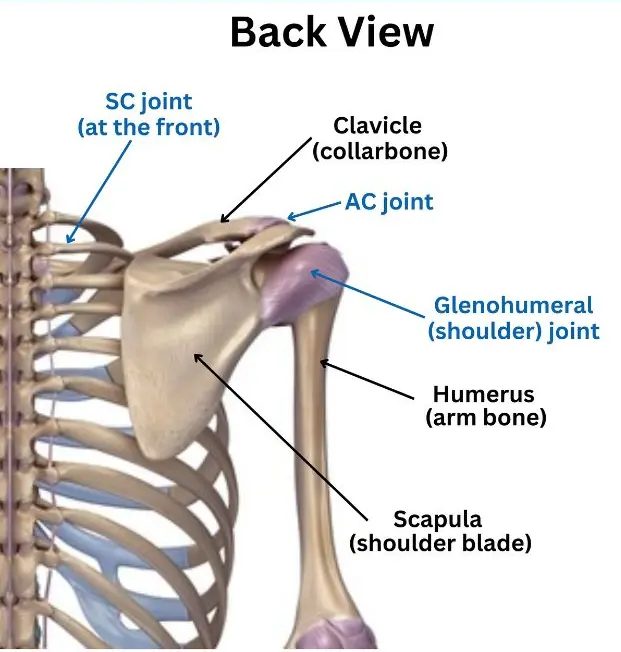
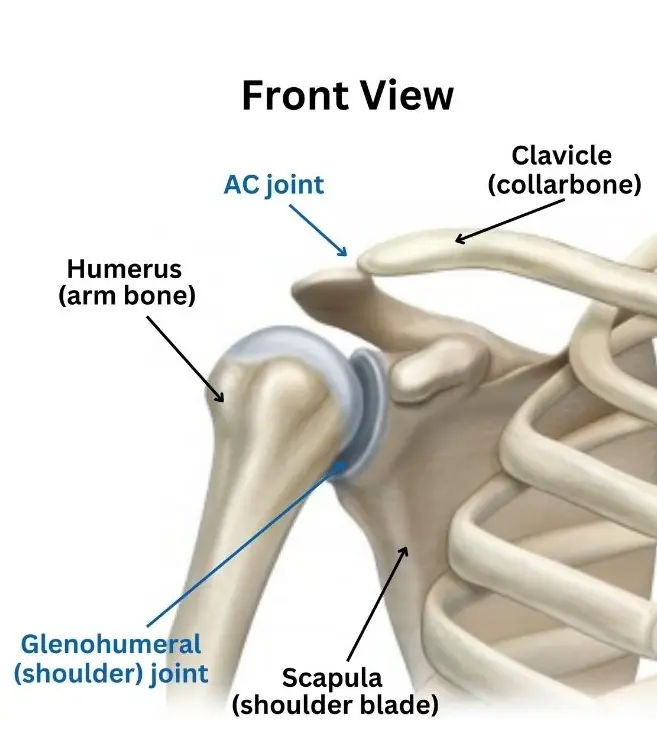
The shoulder complex (girdle) is made up of the shoulder blade (scapula), the collarbone (clavicle) and the arm bone (humerus). The joint we know as the shoulder is formed between the head of the humerus and a socket on the shoulder blade (glenoid fossa). However, movement of the shoulder also involves the AC joint (acromio-clavicular joint) between the collar bone and the shoulder blade, the SC joint (the sternoclavicular joint) between the collar bone and breast bone, and the joint that forms between the shoulder blade and the rib cage (scapulothoracic joint). For optimal shoulder complex function, all of these joints need to move well, along with optimal tone of the associated muscles and good resting position of the bones (in particular the humerus and scapula).
Common findings in the chiropractic clinic with patients with shoulder pain are joint dysfunction and poor resting position and function of the shoulder complex. This is accompanied by tender and tight muscles, particularly the rotator cuff muscles.
Multiple studies have demonstrated an increased risk of soft tissue pathology in the presence of altered shoulder blade positioning.
Scapulothoracic dyskinesis can also occur post injury such as AC joint injuries, rotator cuff tears, fractures of the clavicle, shoulder sprains and impingement. Despite the original injury healing, the effects of scapulothoracic dyskinesis may not become symptomatic for some time.
The Scapula (shoulder blade)
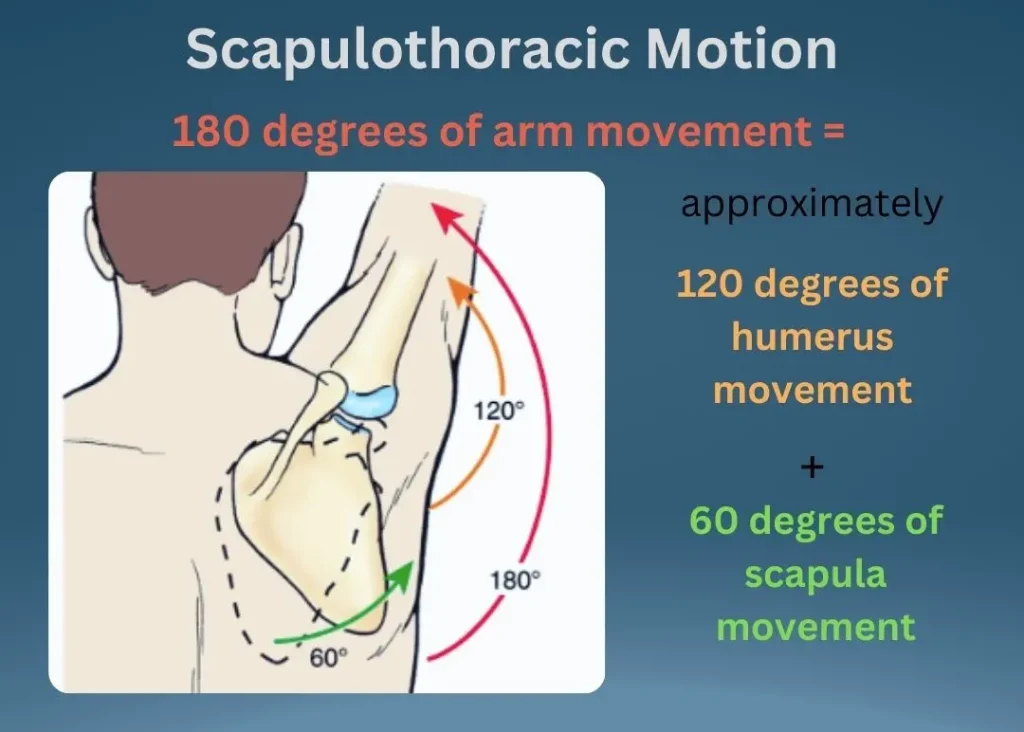
Full shoulder movement requires the shoulder blade to be positioned correctly on the rib cage to allow adequate movement. Aberrant movement within the shoulder complex increases the chance of injury, as other joints and muscles are forced to compensate. This is important in anyone, but more so in athletes who have a higher and more intense use of the shoulder. Abnormal movement of the shoulder blade (scapulothoracic dyskinesis) has been associated with a 43% increased risk of shoulder pain when considering athletes requiring overhead actions. Multiple studies have also demonstrated an increased risk of soft tissue pathology in the presence of altered shoulder blade positioning. There is available research associating altered scapula movement with shoulder impingement, tendinopathy and tears of the rotator cuff, frozen shoulder and joint instability. In these scenarios it has been demonstrated there is also altered muscle function of the associated muscles, particularly those stabilising the shoulder blade.
One of the common causes of altered scapula positioning in the chiropractic clinic is an increased thoracic kyphosis (rounded/hunched middle back), whether structural or muscular in origin. With this posture, the shoulder blade moves out and forward and rotates on the rib cage. This tilted resting position reduces the range of motion of the shoulder (glenohumeral) joint and disrupts the scapulohumaral rhythm required for optimal shoulder movement. The shoulder blade and collarbone then need to work harder to obtain desired shoulder movement. Not only does this place more stress on the involved joints, the associated muscles are placed under stress and the shoulder blade position can begin to impinge structures such as the bursa and the supraspinatus tendon. This process happens over time and can explain the onset of pain in the absence of a specific injury. Scapulothoracic dyskinesis can also occur post injury such as AC joint injuries, rotator cuff tears, fractures of the clavicle, shoulder sprains and impingement. Despite the original injury healing, the effects of scapulothoracic dyskinesis may not become symptomatic for some time.
Treatment
In the chiropractic clinic, given what is known about the complexity of the shoulder girdle and the relationship with posture, treatment will typically focus on posture and spinal function, as well as shoulder girdle function and position, existing or past shoulder pathologies, soft tissue treatment, shoulder and postural exercises and lifestyle.
Chiropractic adjustments aim to improve joint motion and function. Exercises given are targeted at muscle imbalance, posture and stabilisation. It is also important lifestyle habits are addressed that may continue to place stress on the shoulder complex.
How important are shoulder exercises?
Given the importance of the position of the scapula and its movement on the rib cage, it is essential to consider the primary stabiliser of the scapula – the trapezius muscle.
All three sections of the trapezius muscle play an important part of stabilisation, with the upper fibres pulling in upward rotation, the middle fibres pulling the scapula towards the spine and the lower fibres both contributing to downwards rotation and stabilisation when the arm is completely elevated. Imbalance between the upper, middle and lower trapezius can contribute to altered position of the shoulder blade.
Another important muscle for optimal scapula motion is serratus anterior. The primary role of the serratus anterior is stabilising the scapula against the thoracic (rib) cage, preventing excess motion, especially when the arm is stretched across the body.
The other muscles to play a major role in scapular stabilisation are the rhomboids (major and minor) which help the middle trapezius with its role.
Exercises aimed at these muscles will help with optimal scapula position and function.
What does the research say?
- In a 2019 study looking at the effect of manual therapy and stabilising exercises on forward head and rounded shoulder postures, the participants receiving both manual therapy and stabilisation exercises saw the most improvement in function and pain.
- Altered scapular movement has been found in conjunction with a shortened pectoralis minor muscle, tight soft tissue at the back of the shoulder complex and a hunched middle back posture.
- In a systematic review and meta-analysis of the effectiveness of scapula (shoulder blade) focused approaches in patients with rotator cuff related shoulder pain, there was a statistically (but not clinically) significant benefit with respect to pain with scapula focused approaches in the short term (first 6 weeks). There was also a significant improvement in the level of disability with scapula focused approaches in the first 6 weeks.
- Studies have reported anywhere from 68-100 % of patients presenting with shoulder pathologies also present with scapulothoracic dyskinesis.
- Scapulothoracic dyskinesis has been found to be common in those patients complaining of neck and shoulder pain. They often present with shoulder instability and associated muscle weakness.
- While athletes are at a higher risk of developing shoulder injuries, another high-risk group identified are those spending prolonged periods in front of personal computers. Poor posture has been implicated as the cause.
References:
Bury J, West M, Chamorro-Moriana G, Littlewood C. Effectiveness of scapula-focused approaches in patients with rotator cuff related shoulder pain: A systematic review and meta-analysis. Man Ther. 2016 Sep;25:35-42.
Fathollahnejad K, Letafatkar A, Hadadnezhad M. The effect of manual therapy and stabilizing exercises on forward head and rounded shoulder postures: a six-week intervention with a one-month follow-up study. BMC Musculoskelet Disord. 2019 Feb 18;20(1)
Jildeh TR, Ference DA, Abbas MJ, Jiang EX, Okoroha KR. Scapulothoracic Dyskinesis: A Concept Review. Curr Rev Musculoskelet Med. 2021 Jun;14(3):246-254
Ludewig PM, Reynolds JF. The association of scapular kinematics and glenohumeral joint pathologies. J Orthop Sports Phys Ther. 2009 Feb;39(2):90-104.
Saini SS, Shah SS, Curtis AS. Scapular Dyskinesis and the Kinetic Chain: Recognizing Dysfunction and Treating Injury in the Tennis Athlete. Curr Rev Musculoskelet Med. 2020 Dec;13(6):748-756


