Plagiocephaly and developmental delays in children
What is Plagiocephaly?
Positional or deformational plagiocephaly is a condition characterised by an asymmetrical head shape or flattening on one side of the skull. Plagiocephaly can often cause long term changes to the baby’s head shape and can cause facial asymmetry.
Plagiocephaly has become more common in children since the early 1990’s. Around this time the “Back to Sleep†program was being introduced to try and reduce the number of SIDS deaths in infants. (3) This program encouraged parents to put their children to sleep on their back and thus increased the overall time a baby now spends on its back. (3) Researchers have noticed a sharp increase in Plagiocephaly since this program was introduced. (3) The prevalence of plagiocephaly in infants from 7-12 weeks of age is 46.6%. (6)
Risk factors for developing plagiocephaly include: (4)
- Long periods spent on back and reduced tummy time.
- Reduction in neck range of motion – This causes a head preference to one side.
- Instrument delivered infants (forceps or suction).
- Intrauterine constraint (restriction in baby’s movement while developing inutero)
- Twins or multiple births
How do I know if my child has plagiocephaly?
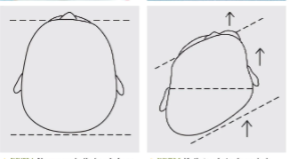
Plagiocephaly presents with a range of severity in head shape changes. The moderate and severe changes are much more easily noticed by the untrained eye and is something you can check for at home (see below for picture of examples).

How to check for plagiocephaly
- Does your baby have a head preference? – Do they always lay facing one side? Do they always hold their head to one side during tummy time?
- Look at your baby’s head from above them – sometimes it is useful to take a photo so you can compare the pictures.
- You are looking for an increase in flatness on one side of the back of the head. You may also notice your baby’s ears don’t line up or their forehead comes forward on one side. (See Picture below) Mild forms are much harder to notice as the ear position and face shape are often unaffected.
If you notice any of these changes then we would advise you getting this checked by your healthcare provider (Chiropractor, Maternal Child Health Nurse, GP).
What the research says about plagiocephaly and developmental delays in children
Current research and literature reviews show a strong correlation between plagiocephaly and developmental delays in children. Most researchers agree that plagiocephaly could be used as a marker of elevated risk of developmental delay. In one study the prevalence of plagiocephaly and developmental delays was as high as 40% (2).
Developmental delays can range from motor delays (late crawling and walking) to learning issues noted later in childhood. Motor delays are most commonly found in children under two and learning delays in children over two.(1)
One study assessing mental and psychomotor development found that infants with plagiocephaly were more likely to show delays in both areas. The study found none of the assessed children were advanced or accelerated in development. 90 percent had normal mental development scores, 7 percent were mildly delayed, and 3 percent severely delayed in mental development. For psychomotor development 74 percent were normal, 19 percent mildly delayed, and 7 percent severely delayed in psychomotor development. Although a large proportion of the children (90% and 70% respectively) showed normal development no child tested with plagiocephaly demonstrated advanced or accelerated development. (5)
Although not all children with plagiocephaly will develop delays it is not clear which children with plagiocephaly will or will not have issues. A large majority of the children assessed in the studies presented with reduced cervical (neck) range of motion. This reduction in movement leads to the child having a head preference and the increase in pressure on that side of the head increases the chance of developing plagiocephaly. If we can correct the reduction in cervical range of motion and therefore reduce the chance of plagiocephaly developing we are giving the child a better chance of normal or accelerated development. Overall it is clear the research recognises the importance of early recognition and correction of plagiocephaly to help improve a child’s development.
How we can help
Chiropractors and well trained to assess a child for reduced cervical range of motion, developmental delays and head shape changes. We utilise a range of gentle and effective treatment approaches to help your child move and function better. Chiropractors can also offer advice and support with activities you can do at home to increase your baby’s movement and development. Correction of plagiocephaly and head shape changes is most effective in the first 6 months of life before your baby’s skull bones start to fuse together. We would recommend having your child assessed by a paediatric trained chiropractor if you notice any of the risk factors above or changes in movement and head shape.
- Martiniuk, Alexandra L. C.; Vujovich-Dunn, Cassandra  ; Park, Miles; Yu, William; Lucas, Barbara R., 2017 ‘ Plagiocephaly and Developmental Delay: A Systematic Review’  Journal of Developmental & Behavioral Pediatrics, Volume 38, Number 1
- Robert I. Millerand Sterling K. Clarren, 2000, ‘Long-Term Developmental Outcomes in Patients With Deformational Plagiocephaly’ Pediatrics February 2000, 105
- Andrews, Brian T. MD, MA; Fontana, Stefani C. PhD 2016 ‘Plagiocephaly and Developmental Delay’ Journal of Craniofacial Surgery: September 2016 – Volume 27 – Issue 6 – p 1381-1382
- BL Hutchison, Alistair W Stewart, Edwin A Mitchell 2009 ‘ Characteristics, head shape measurements and developmental delay in 287 consecutive infants attending a plagiocephaly clinic’ Acta Paediatrica Vol 98 Issue 9
- Kordestani, Rouzbeh K. M.D., M.P.H.; Patel, Shaurin M.D.; Bard, David E. M.S.; Gurwitch, Robin Ph.D.; Panchal, Jayesh M.D., M.B.A 2006 ‘ Neurodevelopmental delays in children with deformational Plagiocephaly’ Plastic and Reconstructive Surgery: January 2006 – Volume 117 – Issue 1 – p 207-218
- Aliyah Mawji, Ardene Robinson Vollman, Jennifer Hatfield, Deborah A. McNeiland Reginald Sauvé 2013 ‘The Incidence of positional plagiocephaly: A cohort study’ Pediatrics August 2013, 132 (2) 298-304


